


A clinical trial is one way to advance colorectal cancer treatment options. But patients –and their doctors also – may think that clinical trials are a last-ditch effort in treatment, and that you need to be stage IV to be eligible. Maia Walker, the lead curator of the Fight CRC Clinical Trial Finder, addresses the top myths about clinical trials.
Clinical trials are available for all patients of all stages.
For instance, there are trials for newly diagnosed patients, exploring non-surgical approaches or combining immunotherapy with surgery to prevent recurrence. There may be research studies focused on patients receiving adjuvant chemotherapy, aiming to mitigate specific side effects associated with the treatment.
Then, when thinking about trials for patients with stage IV colorectal cancer, it’s essential to recognize that they span each line of treatment within the metastatic setting. We saw trials for metastatic disease where an immunotherapy was added to chemotherapy, as part of the first-line therapy. Also, there have been trials for third-line therapy for stage IV cancer that tested the standard-of-care drug at a lower dose than usual, resulting in similar clinical outcomes with fewer side effects.
Some trials specifically target patients who haven’t yet received certain standard-of-care agents (such as cetuximab or regorafenib), providing those with additional treatments/drugs. In summary, clinical trials should not be viewed solely as a last resort for stage IV patients.
Learning requires time.
Understanding the clinical trials landscape is a gradual process. As advocates, we aim to equip patients with relevant information early on, ensuring they don’t miss potential opportunities. Whether patients choose to participate in a clinical trial early, later, or not at all depends on their unique circumstances. Regardless, it’s crucial to make an informed decision.
Including trials in your treatment strategizing opens more options for you early on.
Metastatic or stage IV colorectal cancer, which has spread to other organs, has very few effective treatments. The first and second line of chemotherapy (FOLFOX and FOLFIRI + a biologic) work well initially to shrink tumors and contain their growth.
Unfortunately, most stage IV folks can progress on these regimens and the drugs available as third-line options are not as effective for many patients. Often, patients only realize this after they have progressed on earlier lines of therapy.
Learning about the trial landscape when you have progressive cancer, and your body is beat up from treatments you have received so far, may be much harder when compared to learning about trials when you are doing well on chemotherapy or have stable disease. So, spending the time early on to learn about clinical trials can be very helpful to patients and caregivers to plan out their long-term strategy to deal with colorectal cancer.
Also, you may want to expose yourself to second opinions as you start looking for trials.
As patients search for and learn about trials, it is likely that their understanding of the options available for metastatic colorectal cancer, including local treatments, may expand. They may become aware of options they did not know previously, which may be available at other hospitals, for example. So, even if you don’t end up getting on a trial, your disease trajectory may become much different after learning about and pursuing additional options, like local treatment of specific metastases.
How can I meet other patients and caregivers who are like-minded and looking for trials?
Searching and learning about trials can help you meet other patients and caregivers who are like-minded and help you find and become part of patient communities like Colontown and Fight CRC’s Community of Champions.Your learning experience becomes easier and faster if you can learn from other people’s experiences as well. Like everything else, learning about trials in a community with others like in the Colontown Clinical Trial neighborhoods or learning to use the Fight CRC’s Clinical Trial Finder are ways to make clinical trial search less daunting for patients.
The Colontown University Clinical Trial Basics Learning Center is a great place to learn about clinical trials, as well as the Searching Safari course, which helps patient and caregiver members of Colontown to familiarize themselves with things patients need to consider way before they start their trial search. This course is like dipping your toes in the ocean of trials and can be just the right “training” needed before people dive into using clinical trial finders like the Fight CRC Trial Finder.
When patients begin their stage IV treatment, many are not aware of what lies ahead. This is related to what I wrote earlier. Thinking about trials and how to incorporate experimental therapies as part of their treatment usually comes from an understanding of the treatment landscape and the realization that metastatic colorectal cancer does not have a lot of effective drugs against it.
Patients who learn about trials early on may have a more realistic understanding of the limitations of current standard-of-care drugs. Being aware of the treatment landscape can help patients and caregivers to be proactive and learn to strategize treatment planning. Learning about clinical trials early can make patients more prepared for what lies ahead.
Contemplating clinical trials can provide greater clarity regarding your own decisions and help you navigate the uncertainties inherent in a cancer journey.
Identifying what you don’t want can guide you toward what truly matters. It lets you define both short- and long-term treatment goals and life goals. This clarity significantly aids in the complex decision-making involved in treatment planning.
Recognizing the types of treatments you wish to avoid requires understanding all available options, making early consideration essential for navigating the uncertainties of a cancer journey.
Despite receiving a stage IV colorectal cancer diagnosis, life continues. By directing your efforts toward understanding clinical trials as a proactive choice rather than a reactive necessity, you can regain a sense of empowerment and some control amidst the chaos that accompanies such a diagnosis.
 Karen Desjardins, age 69, is a survivor of four different cancers. She was diagnosed with breast cancer at age 36, colon cancer at age 44, ovarian cancer at age 47, ovarian cancer recurrence at age 49, breast cancer (primary, not a recurrence of the first one) at age 53, and metastatic breast cancer at age 65.
Karen Desjardins, age 69, is a survivor of four different cancers. She was diagnosed with breast cancer at age 36, colon cancer at age 44, ovarian cancer at age 47, ovarian cancer recurrence at age 49, breast cancer (primary, not a recurrence of the first one) at age 53, and metastatic breast cancer at age 65.
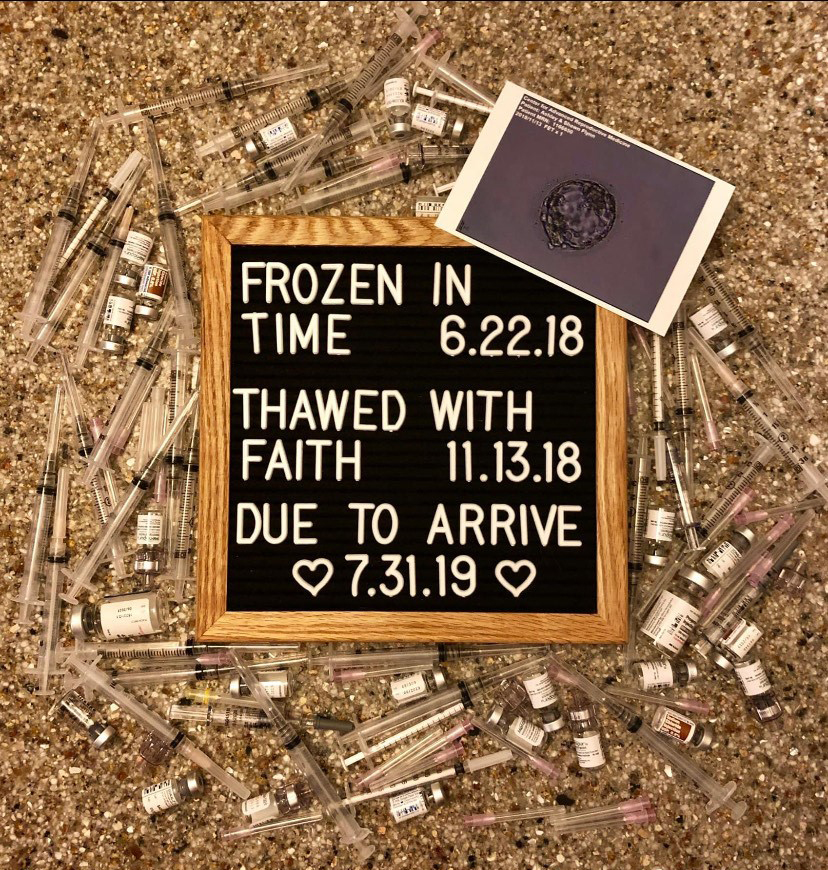 I learned in 2014 that once my ovarian transposition surgery was done, that was it. It couldn’t be reversed. Because of the surgery, we would need to have IVF to have children.
I learned in 2014 that once my ovarian transposition surgery was done, that was it. It couldn’t be reversed. Because of the surgery, we would need to have IVF to have children.
 My dream is every single cancer patient, no matter the diagnosis or age, should have a fertility preservation consult.
My dream is every single cancer patient, no matter the diagnosis or age, should have a fertility preservation consult.